

















A tool to help assess disinvestment in support services can help organisations validate their difficult decisions in this area, as Marion Bain, Hester Ward and Simon Belfer explain.
The NHS spends a significant proportion of its budget on services that support direct, patient-facing services. An estimated 30 per cent of NHS Scotland’s workforce comprises administrative and support staff. While the effects of these support services could be considered indirect, they have a major impact of the quality and efficiency of frontline services.
With tightening budgets, there is increasing pressure for the NHS to prioritise and, when required, to agree on disinvestments. Using combinations of financial, outcomes and ethical frameworks, considerable work has been undertaken to develop valid methodologies to prioritise clinical services.
But it is important that the prioritisation decisions about support services are made using an objective and systematic methodology, which is as robust, valid and open to scrutiny as the methods used for direct clinical services. There is however very little guidance or published information to help health service managers to do this.
NHS National Services Scotland (NSS) is the main provider of national-level support services to NHS Scotland. It deals with national procurement, health protection support, blood transfusion services, provision of information, commissioning of screening and specialist health services, information management and technology services, patient GP registration services, counter fraud services, legal services and facilities support. A methodology was developed within NSS to ensure decisions about prioritisation and disinvestment could be made systematically and objectively, relying on the best available information and evidence, applied in a practical and pragmatic way.
This tool has been put into practice to assist prioritisation, service redesign and efficiency decisions and has now been rolled out for use as a decision assisting tool throughout NSS.
Scoring the Relative Health Impact of different NSS
| Health impact score | Extent of potential health | Number of people positively affected per year | Likelihood of the health impact being realised |
|---|---|---|---|
| 1 (low) | Prevention of minor adverse event Small improvement in health status | <5,000 | Hard to imagine happening |
| 2 | 5,000<50,000 | Unlikely (15-35%) | |
| 3 | Moderate improvement in health status | 50,000<500,000 | Possible (35-60%) |
| 4 | 500,000<5,000,000 | Likely (60-80%) | |
| 5 (high) | Prevention of severe adverse event Significant improvement in health status Prevention of death/long term morbidity | >5,000,000 | Almost certain (80-100%) |
The key steps
Ensure leadership from both a finance and a health perspective: Costs and benefits are equally important when making decisions about priorities. The work in NSS was jointly led by the director of finance and the medical director, which allowed the different expertise and perspectives to influence the methodology’s development.
Engage and involve service managers and providers: While the work was led at executive director level, the managers of the services were involved from the start and began by defining their services. NSS has 10 operating divisions and the directors of each were asked to provide descriptions of their services grouped into a maximum of nine categories. These were described in terms of services to customers. In total, it was agreed that 67 services covered all NSS external services and the managers provided the relevant information to assess the costs and benefits.
Use evidence, good practice and, if needed, new approaches: The basic approach was based on health economic principles with the costs and benefits of each service being assessed. Although identifying the costs of each service was relatively straightforward, assessing benefits was more challenging. NSS services are diverse and, generally, several steps away from the ultimate health or healthcare outcomes for patients.
NSS has categorised the benefits of its services into two broad groups. These are health impact benefits (services that ultimately contribute to improved health outcomes for patients and the public) and financial impact benefits (services that save the NHS money).
The assessment of relative health and financial benefits of each service across our diverse portfolio of services required some innovative thinking. Development work was undertaken in NSS to identify how to measure the relative health impact and financial impact of the range of support services provided.
To assess health impact a methodology was developed and applied by a multidisciplinary clinical group from across NSS. This involved scoring for each service: the extent of potential health impact; the number of people positively affected by the service; and the likelihood of the potential health impact being achieved given the gap between the service and frontline delivery of health services (see table, left).
Scores were agreed for each service and multiplied together to obtain a relative health impact score. The importance of comparing relative rather than absolute scores was recognised (the absolute scores in themselves carried little meaning). To aid this comparison and prevent potentially invalid discussions of absolute scores, the scores were then divided into three categories to define the health impact of each service as high, medium or low.
To assess financial impact, an approach was developed that assessed the cost avoidance of providing a service once for the whole of NHS Scotland rather than numerous times, as well as cost savings that reflect additional savings generated for NHS Scotland. This was done by a service examining its scope and activities, and providing them at a lower cost for both itself and NHS Scotland (see table, below right). These two aspects were combined and the overall financial impact of each service was categorised as high, medium or low.
Consider factors beyond the obvious costs and benefits: Although costs and benefits form the basic information for prioritisation decisions, it would be naive to think decisions on service provision will depend on these alone. For the NSS some services are required by statute, others are provided to meet a legal requirement and some are driven by political commitments. Whether or not these factors applied to each of the NSS services was considered. In addition, the practical likelihood of a reduced or discontinued service actually freeing up resources was assessed.
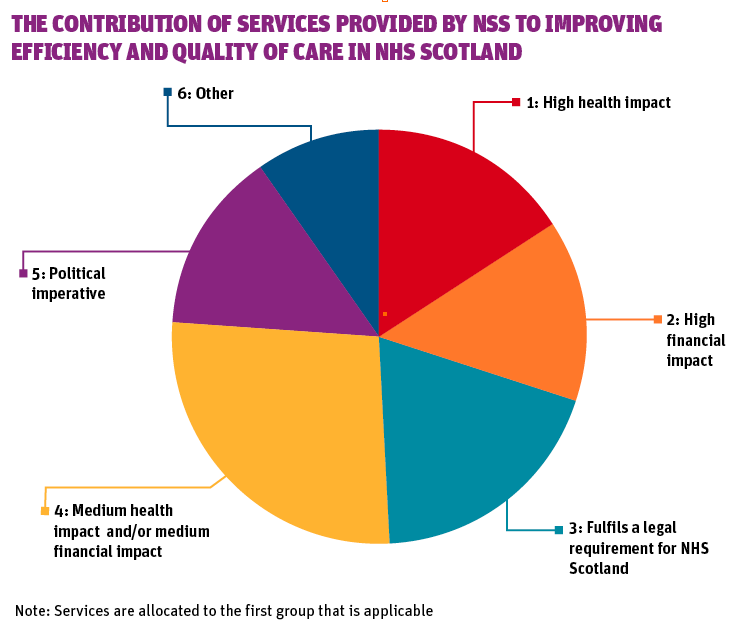
Start using the information as soon as it is fit for purpose: The work outlined here resulted in detailed spreadsheets containing information for all 67 services. We were able to use this as soon as it was collated to perform an initial high level review of these services. In particular, we used it to assess to what extent each one met the NSS agreed mission and purpose, and to what extent each one contributed to improving quality of care and efficiency for NHS Scotland (view diagram).
We also used the information to identify potential groups of candidate services for efficiency measures, service redesign and disinvestment, based on an informed decision balancing costs and benefits, which formed the basis of further discussion with service managers.
The results of the tool were used in discussion with external stakeholders, which gave an opportunity for peer review and endorsement of the tool’s use and validity. Although the information was used as soon as it was available, it was recognised that improvements could, and should, be made. NSS managers were encouraged to use the methodology to assess their services in more detail and feed back improvements.
Categorisation of the Relative Financial Impact of different NSS Services
Financial impact per year COST AVOIDANCE | Financial impact per year ACTUAL SAVINGS |
|---|---|
| Low: <£0.5m | Low: <£1m |
| Medium: £0.5-5m | Medium: £1m-£5m |
| High: >£5m | High: >£5m |
A basis for discussion
It is important to note that the whole approach is based on understanding the relative costs and benefits of services, as opposed to their absolute values. Although some quantifiable measures were used, much of the approach reflects qualitative assessments (that is, high, medium and low ratings), with the aim of providing a practical and achievable approach to robustly differentiating services. This can lead to further detailed work and discussions on a smaller subset of services as and when required.
We believe this approach has potential for wider applicability, in particular to support comparisons and decision making across diverse services that indirectly support clinical care.
Focusing on how support services improve quality and reduce costs allows their contribution to be recognised and, ultimately, to be developed so it can be increased.
Although the methodology does not produce definitive answers, it provides a robust, objective and explicit basis for discussion with stakeholders about the value and prioritisation of support services that, to date, have been very difficult to compare in a meaningful way.



{kind=link}
1 Readers' comment