
















Developing a successful acute oncology service to admitted patients and those in A&E called for some innovative thinking, explain Rob Smith and colleagues.
At Clatterbridge Cancer Centre Foundation Trust we have developed a new service for acute oncology, together with the local cancer network. It provides a network of acute oncology consultants based between all the acute hospitals in the Merseyside and Cheshire cancer network. The service provides on-call and daily support to inpatient as well as accident and emergency wards.
The requirement for the service represented a significant challenge – namely, how to provide a 24/7 acute oncology service that was local to the acute hospitals while also being part of the specialist network of services provided out of Clatterbridge Hospital.
Through collaborative working between Clatterbridge, the cancer network, commissioners and acute hospitals, it has been possible to establish a service that improves both patient care and efficiency.
Patients attending A&E with cancer have traditionally received a poor service; a lack of specialist oncology skills in A&E has led to poor diagnosis and lack of treatment within that department. Patients were often admitted unnecessarily then passed between specialties, experiencing long delays before diagnosis and treatment.
Patients attending A&E for the first time would typically be late to present with symptoms and already in the latter stages of disease progression. Confusion around their diagnosis and treatment increased anxiety for them and their carers.
The problems with these services were recognised in the National Confidential Enquiry into Patient Outcome and Death’s For Better or Worse, and a report from the National Chemotherapy Advisory Group report recommending the establishment of an acute oncology team in each trust with an emergency department by 2011 at the latest.
Peer review measures for acute oncology have now clarified the requirements from each acute hospital including:
- an acute oncology team, including A&E, acute medicine and oncology;
- consultant oncology assessment within 24 hours of admission;
- protocols for treatment of acute oncology presentations.
Oncology services across the network are provided by Clatterbridge in partnership with local acute providers. Each hospital has a chemotherapy service on site, which is provided by visiting Clatterbridge oncology consultants, who also attend local multidisciplinary team meetings.
Getting off the ground
The service was supported by chemotherapy nurses and funded through service level agreements between the foundation trust and the acute hospitals. An acute oncology service had been piloted in St Helens and Knowsley Teaching Hospitals Trust.
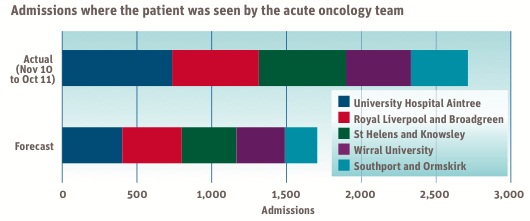
The strong network structure and collaboration between the trusts were central to providing a framework for the solution. A proposal was developed jointly between Clatterbridge and the cancer network, which described a new acute service to the acute hospitals and commissioners. Required resources are shown in the table (below); the number of potential admissions per hospital, calculated on the basis of hospital episode statistics, Clatterbridge activity data and the cancer registry, are shown in this graph.
Resource requirements
| Resource type | Requirements |
|---|---|
| Oncology consultant | 2 per hospital; an additional 5 oncologists required |
| Nurse specialist | 1 whole time equivalent (or 2 part time) for each hospital |
| Secretary | 0.5 per hospital |
Admissions were separated into three categories:
- new cancer patients;
- post-chemotherapy/radiotherapy complications;
- known cancer complications.
No additional funding was available to support the development and local NHS budgets were being significantly reduced; as such, finding the resources for this development would be challenging.
This issue was dealt with by identifying a potential reduction in length of stay for patients as a result of the improved patient pathway. The cost per hospital would be compensated through reduced bed costs.
The acute hospitals predicted difficulties in “cashing in” these benefits in the context of increases in other acute demands. It was agreed the primary care trusts would provide pump priming funding using commissioning for quality and innovation money. The service could then become established and the benefits demonstrated.
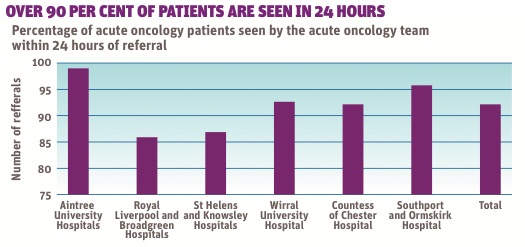
The service was implemented throughout 2010–11 and has been reviewed with regard to:
- patients reviewed in 24 hours;
- total activity against plan;
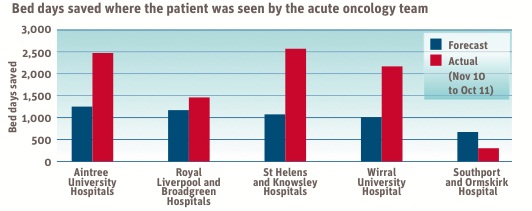
- length of stay reduction;
- feedback from lead cancer clinicians.
A telephone audit of feedback from lead cancer clinicians has brought positive feedback. All the hospitals that responded confirmed good progress on protocol development. There was a general view that the acute oncology service had also made a general improvement to the cancer team. As one responder explained: “I don’t know how we managed without it!”
From ‘if’ to ‘how’
The project is achieving all of the main objectives; patients are being seen within 24 hours in most cases and length of stay has been reduced. The activity level is above plan and the protocols are in place in most areas. As a result of its success, the service is now recognised as essential and the debate has moved on from “if” it is required to “how” the funding mechanism for it will operate.
The activity predictions have proved accurate and length of stay reductions have been achieved. However, the scale of bed day reductions is small in relation to large acute hospitals, and calculating the financial benefit is challenging.
The financial model has been adapted to show the marginal income gain from increased admissions into the beds vacated by the patients with cancer. On this basis it is still possible to show a financial gain from the model. The funding mechanism is still being discussed between the commissioners and acute providers.
The service is still in development and work is continuing on further improving protocols and working practices. There may also be opportunities to improve service integration between primary care, acute hospitals and specialist oncology. The new acute oncology team is looking to work with colleagues in acute hospitals and primary care to identify further service improvements to this group of patients.
Also online
What makes an excellent foundation trust? Colleagues from consultancy Finnamore revealsthe results of a survey of chief executives designed to get a ‘snapshot’ of their thinking on some key questions on what makes a foundation trust excellent.






{kind=link}
{kind=link}
{kind=link}
No comments yet