
















A foundation trust is pioneering significant improvements in the clinical handover of patients, writes Catherine Boereboom.
A patient’s journey through hospital from admission to discharge involves different physical places and input from many different staff, working different shifts.
With so many links in the chain there is huge potential for incomplete or hasty handovers and consequent errors. It is imperative that patient information is handed over to successive, responsible medical personnel in a timely and comprehensive manner.
Successful clinical handover must involve a system that is standardised and easy to use.
Sherwood Forest Hospitals Foundation Trust, which runs King’s Mill Hospital in north Nottinghamshire, believes the key to success is in actively involving frontline staff in making improvements. Its approach has been tagged “Achieving Best Care”.
ABC is a service improvement and organisational development framework that supports the delivery of the trust’s pledges as well as its strategic and business objectives. ABC seeks to deliver sustainable quality and productivity benefits. The solution embraces employee engagement, innovation and the application of best practice in lean thinking.
This clinical handover project illustrates how a thorny problem faced by many acute teams can be addressed through dialogue, the use of improvement methodologies and a joined-up approach to people, process and technology.
Traditionally, clinical handover might have entailed a mix of verbal conversation, telephone messages via bleep systems, handwritten notes or collections of patient identity stickers on printed proformas.
As more advanced communication technology has established its place in healthcare, personal digital assistants and other mobile communication devices are being used to hand over clinical tasks.
Negative feedback from junior surgical staff prompted a review of the way clinical tasks were being handed over between were not being completed when they were requested, and many clinically necessary tasks were being discovered incidentally during routine weekend ward rounds.
Executive medical director Nabeel Ali explains: “There were too many inconsistencies creeping in, so we needed to find out what was at the root of the problem and change it.
Significant concerns for patient safety were voiced and analysis clarified that clinical handover was a consistent contributory factor. There was lack of a clearly documented, auditable, standardised approach for teams and individual doctors to follow.”
A surgical specialty registrar led the ABC handover project. A project team was established with representatives from service improvement, IT, information governance, patient safety, operations and clinical staff to tackle the challenge of improving handover. The development of the system was also guided by regular dialogue with senior medical leaders. This ensured the all-important sponsorship and support was demonstrated at a senior level.
Consultation with junior doctors and the hospital at night team identified a shortlist of options for improvement (see suggested improvements, below).
This included formalised handover meetings, a computerised system that tracks patient movement and tasks throughout their inpatient stay, and colour-coding to help prioritise different tasks.
It was agreed that the ideal handover system would be an easy to use, computerised list that was accessible from all hospital computers and made task requirements and priorities easily visible. It should track the handing over and completion of medical tasks. And it also needed to highlight the results of out-ofhours tasks to the parent team.
Given that the trust’s patient administration system is to be replaced, it was agreed that the new handover system would provide an interim solution, prior to it being integrated into the new PAS. The new process for the ABC clinical handover was introduced at a surgical department meeting and via an online user guide targeting all clinical staff.
Initial teething problems included doctors failing to update the handover list with the results of tasks. The results were being recorded in the patient’s medical notes but not consistently updated on the list.
Doctors were also forgetting to remove handover tasks the following morning, leaving some tasks on the list for the following night shift. Plan-do-study-act cycles were used to test ways of increasing junior doctors’ engagement and compliance with the new handover process.
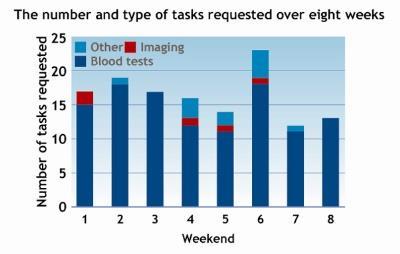
The pilot phase continued with number and type of tasks requested being logged over several weeks (see graph). Further consultation with junior doctors resulted in minor changes to the list throughout the pilot period.
Balancing measures were sought from a survey of the junior doctors (see measures of success, below).
The new handover system and the improvements it brings will be sustainable because it delivers additional benefits for junior doctors. These include:
- improved clinical care of patients;
- an organised list of clinical tasks required during all out of hours periods;
- reliability that all tasks handed over will be completed.
Dr Ali comments: “It’s been a huge benefit to have the junior doctors involved right from the start. They were able to tell us first hand what needed to improve and also what should be implemented to improve the quality and safety of clinical handovers. A great example of junior doctors identifying problems and solving them; I’m really impressed.”
The only additional costs for the new handover system were the time and effort from all those involved in its development, as all computer hardware and software was already in use on the wards.
Our vision for the future is a computer-based, standardised, audited and well-tested handover system, which is used hospital wide to provide comprehensive, timely and reliable exchange of clinical details. It will improve the safety of this potentially risky area of patient care. The outcomes of this improvement project in surgery will form the basis for this system.
Catherine Boereboom is a specialty registrar in general surgery at King’s Mill Hospital.
Handovers: suggested improvements
- More comprehensive patient information needed on list.
- One patient list that tracks patients through their whole stay, via central computer system.
- Colour code urgency of jobs/reviews needed.
- A more complete handover list.
- Patient locations must be correct and up to date.
- Need to be able to specify which grade doctor reviews patients at a weekend. Courtesy calls to covering consultants still appropriate but can be added to list with “consultant review” as a reminder.
ABC: Measures of success
- 87 per cent of surgical junior doctors say the new handover system is easier to use.
- 80 per cent of surgical junior doctors say handover now takes less than five minutes.
- 20 per cent say the handover updates take less than five minutes, 50 per cent take 10-15 minutes, 20 per cent take 15-30 minutes.
- 80 per cent feel more confident out-of-hours jobs will get done.
Find out more
For more information about the ABC handover project please contact Ian Hall, director of service improvement. ian.hall@sfh-tr.nhs.uk



No comments yet