

















An enhanced recovery pathway at a London trust has led to benefits including earlier discharge for patients. Lisa Hollins and colleagues explain how they did it.
In 2010, University College London Hospitals Foundation Trust set out to identify all parts of the elective care pathway – across institutional boundaries – that could be developed to support better preparation and recovery of patients.
Our teams used the elements of this “enhanced recovery” pathway to identify opportunities to develop services and worked with our patient governors to redesign care at each pathway stage.
- Exclusive online extras: see the three documents attached in ‘Related Files’
There are a number of key elements in the enhanced recovery pathway that improve patient experience and outcomes. Of its 17 general principles, 14 need the collaboration of patients (see box, below). It is crucial to work with patients to give them the advice and support they need to prepare themselves for surgery and recovery afterwards.
Just over two years ago, UCLH prioritised the need to accelerate transformation of services and set up its quality, efficiency and productivity programme, which manages large changes across the organisation.
A key pillar of efficiency is enhancing inpatient services and we have focused on elective pathways. We have a trust-wide ward efficiency steering group, led by a medical director and supported by project managers. It oversees improvements to inpatient care and works with clinical teams to deliver change.
Examples of issues the group tackles include discharge before 11am, same day admission, integrated community services and pre-assessment. Patients are on the steering group and have been involved in the design of changes to pathways.
Staff believed they could dramatically transform patient experience and outcomes for elective surgery by further developing enhanced recovery principles to transform every part of the patient pathway.
Following a trust learning event in 2010, a number of surgical specialties showed an interest in enhanced recovery and so a trust wide initiative with patient representatives was established. We worked across multidisciplinary teams to identify the enhanced recovery elements we could develop and integrated them in other trust efficiency projects.
Initiatives included the following:
- We involved patient governors in the rollout and management of the change programme and this continues through the ward efficiency steering group.
- We worked with our local arthritis and musculoskeletal alliance patient group to gain more perspectives on the patient experience and asked for their input to MSK patient information and education.
- We explored and evaluated patient and staff experiences from the colorectal enhanced recovery pathways with focus groups. The focus groups showed that patients and staff understood what enhanced recovery meant and felt the surgical pathway did now follow the enhanced recovery principles. We listen to patient feedback and it has been reflected in pre-assessment information on the ward round process and how patients receive information after their surgery.
- With patients, we designed education tools for self-care management. The tools include general and surgery-specific information leaflets, patient diaries, patient top tips, patient education groups and a patient education film, which is now in its final stages.
- We used evidence to transform care with “chewing gum on prescription” – chewing gum cuts the risk of post-operative ileus (bowel obstruction) in colorectal surgery. Patients in pre-assessment were told about this use of gum and so expected it to be prescribed post-operatively.
- We implemented same-day admission for elective surgery specialties that admitted patients the day before surgery. This change in practice was communicated with patients at the decision making stage of their surgery and the process of pre-assessment outpatient clinics and same-day admission was explained.
Culture shift
Over time, we observed a shift in culture among staff and patients that has impacted on patient care. Culture shifts include the following:
- Patients have been empowered and their expectations managed. The education sessions led by senior staff allow patients to understand the enhanced recovery programme and the expectations of others in the team.
- Patient confidence in discharge planning has increased as they know they will get a telephone call within a week, or appropriate therapy follow-up.
- Self-directed patient engagement has helped to manage care during the hospital stay and plan their care following discharge.
- A change in multidisciplinary team culture has promoted discharge planning, including setting the expected date for discharge in pre-assessment and on admission. The approach to discharge planning is becoming consistent among clinicians.
We applied the core principles of enhanced recovery across the care pathways before, during and after elective surgery which led to patient centred quality care with safe and effective improvements in patient experience. It also improved multidisciplinary team efficiency, reduced waste of resources and reduced length of stay.
Improvements in clinical care include the following:
- multidisciplinary team protocol-led care pathways were reviewed and implemented;
- a joint recovery school forum for pre-assessment for arthroplasty patients;
- an increased post operative physiotherapy service for arthroplasty patients;
- same day pre-admission clinics and education sessions;
- proactive written patient information;
- additional ward information, which includes guidance to patients on whom to contact and when;
- ward floor “feet stickers”, to encourage patients to move around independently.
Improvements across multidisciplinary teams include the following:
- a ward-based steering group to coordinate the care pathway;
- the start of the development of staff educational tools such as e-learning modules.
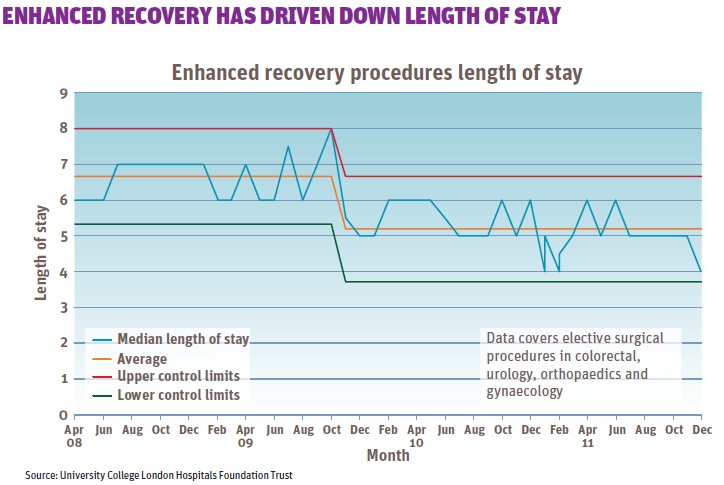
We have seen a steady fall in median length of stay across the enhanced recovery surgical procedures. The specialties included within this measurement are colorectal, urology, orthopaedics and gynaecology. We have also achieved 92.11 per cent same-day admission for 2011-12.
The implementation of enhanced recovery has led to numerous benefits – most importantly an improved pathway for patients where they are ready for discharge earlier.
The feedback from patients on their experience has been overwhelmingly positive and UCLH is supporting patients through pathways more effectively. Reducing length of stay is also positive for the trust. Ultimately, we have delivered better care for patients undergoing surgery.
What patients said
“You don’t realise how daunting coming into hospital and having surgery is; sitting in the group, I saw other patients and I felt that I was not the only person going through this, and I felt reassured. When I came in to hospital and recognised some of the patients that were in the group it gave me courage as I knew I was not alone.”
“It was very personal to me that I had a one-to-one, feeling engaged with somebody who I would be seeing again… I just thought I was in the right place and I was in the right people’s hands.”
“The enhanced recovery… gave me a point of contact for my nursing care who helped coordinate certain issues being resolved and getting out earlier, which was very positive. Some of the individual nurses and care assistants were brilliant and made a real difference to feeling on the ward.”
Key elements of Enhance Recovery from National Enhance Recovery Partnership 2011
| Key Elements of Enhanced Recovery | Patient Involvement(Y/N) | |
| 1 | Optimising the pre-operative health state, commencing in primary care | Y |
| 2 | Anaesthetic Pre-admission assessment with medical optimisation, risk stratification and discharge planning | Y |
| 3 | Preoperative therapy /nursing education eg, Physiotherapy, Occupational Therapy, Nutrition,, stoma care | Y |
| 4 | Informed decision making and managing patient expectations | Y |
| 5 | Admission on day of surgery | Y |
| 6 | Carbohydrate loading and avoidance of dehydration pre-operatively | Y |
| 7 | Individualised intraoperative goal directed fluid therapy | N |
| 8 | Use of short-acting anaesthetic agents | N |
| 9 | Minimal access surgery when possible | N |
| 10 | Minimal or no use of drains/tubes where no supporting evidence | Y |
| 11 | Avoidance of postoperative opiates when possible | Y |
| 12 | Active early planned mobilization | Y |
| 13 | Early removal of catheters | Y |
| 14 | Early removal of IV fluids | Y |
| 15 | Early post-operative oral hydration and nutrition | Y |
| 16 | Procedure-specific daily goals | Y |
| 17 | Discharge once predetermined criteria met and patient in agreement | Y |






{kind=link}
No comments yet